|
Overview
 The best thing to say about the natural history of bunions is that they are unpredictable. This is both in terms of whether the bunion deformity will progress, and also whether the bunion will become painful (if it is not already painful). It would probably however be true to say that once a previously painfree bunion has started to become painful it is not common for the bunion to go back to being entirely pain-free. The best thing to say about the natural history of bunions is that they are unpredictable. This is both in terms of whether the bunion deformity will progress, and also whether the bunion will become painful (if it is not already painful). It would probably however be true to say that once a previously painfree bunion has started to become painful it is not common for the bunion to go back to being entirely pain-free.Causes Bunions can be caused by the following factors. Hereditary (especially via the female line). Rolling in (pronation) of the feet. Walking with turned out feet. Weakness of muscles controlling the big toe. Weakness of intrinsic muscles of the feet. Leaning on the big toe in a tendu, especially to second or derri?re. Reduced mobility of the big toe when on demi-pointe. Restricted pointe range. Symptoms The signs and symptoms of a bunion include a bulging bump on the outside of the base of your big toe, swelling, redness or soreness around your big toe joint, Thickening of the skin at the base of your big toe, Corns or calluses, these often develop where the first and second toes overlap, persistent or intermittent pain, restricted movement of your big toe. Although bunions often require no medical treatment, see your doctor or a doctor who specializes in treating foot disorders (podiatrist or orthopedic foot specialist) if you have persistent big toe or foot pain, a visible bump on your big toe joint, decreased movement of your big toe or foot, difficulty finding shoes that fit properly because of a bunion. Diagnosis When an x-ray of a bunion is taken, there is usually angulation between the first metatarsal bone and the bones of the big toe. There may also be angulation between the first and second metatarsal bones. These angular irregularities are the essence of most bunions. In general, surgery for bunions aims to correct such angular deformities. Non Surgical Treatment One of the best things you can do is to go for wider, deeper shoes. Trevor Prior says there should be a centimeter between the end of your longest toe and end of shoe. You should also choose shoes with an adjustable strap or lace. Podiatrists often recommend exercises to strengthen muscles and tendons around the big toe. Here?s one you can try yourself. Put your feet side by side, and try to move your big toes towards each other. Do this three or four times a day, while you?re in the bath or in bed.  Surgical Treatment If the conservative options fail, your doctor will determine the best surgical procedure based on the severity of your condition. The most common surgical procedure is a bunionectomy, which includes removing swollen tissue from around your big toe joint. Removing part of the bone to straighten your big toe. Realigning the metatarsal bone to reduce angular deformity. Joining the bones in a corrected position to permanently correct the deformity. Most people can get up and walk around the day after bunion surgery, but full recovery can occasionally take up to eight weeks or more. Doctors stress the importance of wearing proper shoes, especially after treatment, to prevent recurrence. If you are at higher risk or prone to bunions, you may not be able to avoid recurrence. Prevention The simplest way to reduce your chance of developing foot bunion or bunionette problems is to wear good-fitting shoes. Avoid high heels as they push your feet forwards to the front of the shoe where they get squashed. Also avoid narrow fitting shoes, especially those that are pointed at the front with a narrow toe box as again, these place pressure through the toes pushing them inwards. Shoes should be comfortable and leave enough room for you to wiggle your toes. Remember, bunions rarely affect non-shoe wearing people. Exercising your feet can also help. By strengthening the foot muscles you can improve your foot position which can help reduce foot bunion problems. Simple exercises like picking up small objects with your toes can help. Overview
When the ankles over-pronate, it throws everything out of alignment. The bones in the feet can actually shift over time, and the muscles and tendons in the leg and ankle will twist. This places repetitive stress on the ligaments, tendons, joints and muscles of the foot, which can cause injury. If your feet are over-pronating, you may notice your muscles feet unusually tired when you way or stand, or they may ache. But symptoms will vary by your weight, age and activity.  Causes Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding additional stress to other parts of the foot. Therefore over-pronation can often lead to a case of Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. People with flat feet often do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves. Symptoms Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful. Diagnosis Look at your soles of your footwear: Your sneaker/shoes will display heavy wear marks on the outside portion of the heel and the inside portion above the arch up to the top of the big toe on the sole. The "wet-foot" test is another assessment. Dip the bottom of your foot in water and step on to a piece of paper (brown paper bag works well). Look at the shape of your foot. If you have a lot of trouble creating an arch, you likely overpronate. An evaluation from a professional could verify your foot type.  Non Surgical Treatment Supportive orthotics in the shoe is a method commonly implemented to treat many common running injuries associated with pronation. An advantage of orthotics is that they often allow the sufferer to continue to participate in athletic activity and avoid other treatment options that could be potentially costly and time consuming. Seventy-five percent of injured runners are successfully treated with the prescription of orthoses. Orthotics are the most effective treatment for symptoms that develop from unusual biomechanics within the body such as overpronation, resulting in either great improvement or complete healing of the injury in about half the cases. Prevention Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot. Overview
Sever condition is an inflammation of the growth plate of the bone at the back of the heel (apophysitis of the calcaneus). The inflammation of Sever condition is at the point where the Achilles tendon attaches to the back of the heel bone. Causes Sever?s disease is common, and typically occurs during a child?s growth spurt, which can occur between the ages of 10 and 15 in boys and between the ages of 8 and 13 in girls. Feet tend to grow more quickly than other parts of the body, and in most kids the heel has finished growing by the age of 15. Being active in sports or participating in an activity that requires standing for long periods can increase the risk of developing Sever?s disease. In some cases, Sever?s disease first becomes apparent after a child begins a new sport, or when a new sports season starts. Sports that are commonly associated with Sever?s disease include track, basketball, soccer, and gymnastics. Children who are overweight or obese are also at a greater risk of developing this condition. Certain foot problems can also increase the risk, including. Over pronating. Kids who over pronate (roll the foot inward) when walking may develop Sever?s disease. Flat foot or high arch. An arch that is too high or too low can put more stress on the foot and the heel, and increase the risk of Sever?s disease. Short leg. Children who have one leg that is shorter than the other may experience Sever?s disease in the foot of the shorter leg because that foot is under more stress when walking. Symptoms Sever's disease causes pain and tenderness in the back and bottom of the heel when walking or standing, and the heel is painful when touched. It can occur in one or both feet. Diagnosis Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain. Non Surgical Treatment It is important that those with Sever?s Disease are treated by a medical professional to reduce pain and allow children to continue to participate in sporting activities. The Athlete?s Foot recommends a visit to your local medical professional to be diagnosed correctly and receive specialised care. Symptoms include pain through the back of the heel where the Achilles tendon inserts into the heel bone, pain during activity especially running and jumping and the back of the heel may be tender to touch.
Overview
 The Achilles tendon, or calcaneal tendon, is a large ropelike band of fibrous tissue in the back of the ankle that connects the powerful calf muscles to the heel bone (calcaneus). Sometimes called the heel cord, it is the largest tendon in the human body. When the calf muscles contract, the Achilles tendon is tightened, pulling the heel. This allows you to point your foot and stand on tiptoe. It is vital to such activities as walking, running, and jumping. A complete tear through the tendon, which usually occurs about 2 inches above the heel bone, is called an Achilles tendon rupture. The Achilles tendon, or calcaneal tendon, is a large ropelike band of fibrous tissue in the back of the ankle that connects the powerful calf muscles to the heel bone (calcaneus). Sometimes called the heel cord, it is the largest tendon in the human body. When the calf muscles contract, the Achilles tendon is tightened, pulling the heel. This allows you to point your foot and stand on tiptoe. It is vital to such activities as walking, running, and jumping. A complete tear through the tendon, which usually occurs about 2 inches above the heel bone, is called an Achilles tendon rupture.Causes As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are corticosteroid medication (such as prednisolone), mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing?s syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture, for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE) - lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60. Symptoms The classic sign of an Achilles' tendon rupture is a short sharp pain in the Achilles' area, which is sometimes accompanied by a snapping sound as the tendon ruptures. The pain usually subsides relatively quickly into an aching sensation. Other signs that are likely to be present subsequent to a rupture are the inability to stand on tiptoe, inability to push the foot off the ground properly resulting in a flat footed walk. With complete tears it may be possible to feel the two ends of tendon where it has snapped, however swelling to the area may mean this is impossible. Diagnosis If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis. Non Surgical Treatment The other option is to allow your tendon to heal without surgery. In this case, you also need to wear a cast, splint, walking boot, or brace for 6-8 weeks. You also may have different exercises to do. If you are less active or have a chronic illness that prevents surgery, this option may be better for you.  Surgical Treatment There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down. Prevention The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics.
Overview
Most flat feet are not painful, particularly those flat feet seen in children. In the adult acquired flatfoot, pain occurs because soft tissues (tendons and ligaments) have been torn. The deformity progresses or worsens because once the vital ligaments and posterior tibial tendon are lost, nothing can take their place to hold up the arch of the foot. The painful, progressive adult acquired flatfoot affects women four times as frequently as men. It occurs in middle to older age people with a mean age of 60 years. Most people who develop the condition already have flat feet. A change occurs in one foot where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Why this event occurs in some people (female more than male) and only in one foot remains poorly understood. Contributing factors increasing the risk of adult acquired flatfoot are diabetes, hypertension, and obesity.  Causes Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors. Symptoms In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot. Diagnosis The diagnosis of tibialis posterior dysfunction is essentially clinical. However, plain radiographs of the foot and ankle are useful for assessing the degree of deformity and to confirm the presence or absence of degenerative changes in the subtalar and ankle articulations. The radiographs are also useful to exclude other causes of an acquired flatfoot deformity. The most useful radiographs are bilateral anteroposterior and lateral radiographs of the foot and a mortise (true anteroposterior) view of the ankle. All radiographs should be done with the patient standing. In most cases we see no role for magnetic resonance imaging or ultrasonography, as the diagnosis can be made clinically. Non surgical Treatment Treatment of Adult Acquired Flatfoot Deformity depends on the stage of progression, as mentioned above paragraphs. Below we will outline a variety of different treatment options available. Orthotics or bracing. To give your foot the arch the support it needs, your podiatrist or foot specialist may provide you with over the counter brace or a custom orthotic device that fits your shoe. Casting. In some cases, a cast or boot is worn to stabilize the foot and to give the tendon time to heal. Physiotherapy. Ultrasound treatments and exercises may help rehab the tendon and muscles. Medications. Over-the-counter (NSAIDS) such as ibuprofen can help reduce pain, inflammation and swelling associated with AAFD. Shoe Gear. Your podiatrist may suggest changes with your shoes you are wearing and inserts you need in your shoe to help support your arch. 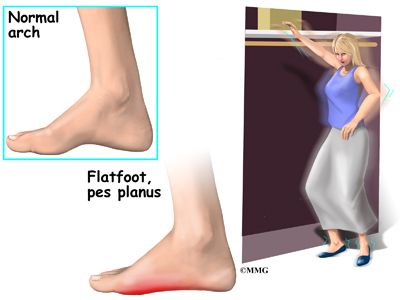 Surgical Treatment Surgery should only be done if the pain does not get better after a few months of conservative treatment. The type of surgery depends on the stage of the PTTD disease. It it also dictated by where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. Some of the common surgeries include. Tenosynovectomy, removing the inflamed tendon sheath around the PTT. Tendon Transfer, to augment the function of the diseased posterior tibial tendon with a neighbouring tendon. Calcaneo-osteotomy, sometimes the heel bone needs to be corrected to get a better heel bone alignment. Fusion of the Joints, if osteoarthritis of the foot has set in, fusion of the joints may be necessary. |
